Author: Kim A. Henderson, PhD, Nicholas Ether, PhD, and Hugo M. Vargas, PhD on September 23, 2025 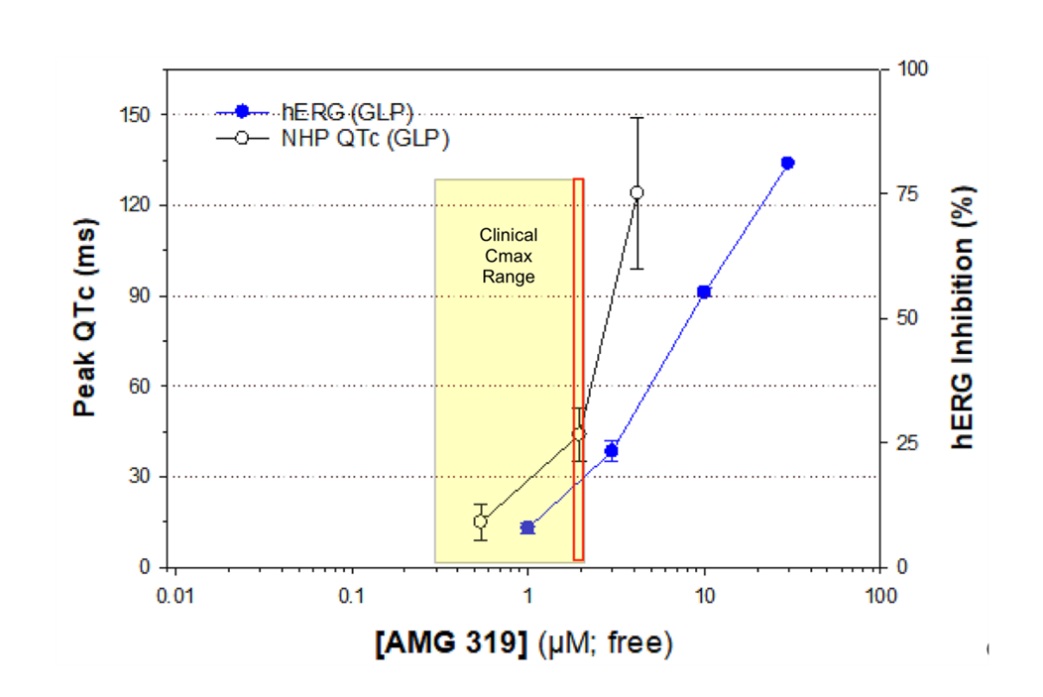
Identifying cardiovascular (CV) risks early in drug development is essential, especially for detecting arrhythmias and hemodynamic changes. Despite this, many nonclinical toxicology studies still rely on brief, restraint-based ECG and blood pressure measurements that often miss the timing of peak drug effects. In our recent study, we compared the sensitivity of these restraint methods to telemetry (the gold standard) across two investigational compounds: AMG 319, a PI3Kδ inhibitor, and AMG 337, a MET inhibitor. In telemetry-based studies, compounds showed clear, clinically meaningful QTc prolongation or hypotension, respectively. However, use of restraint-based method missed the CV effects entirely or inaccurately when compared to nonclinical telemetry and to clinical findings.
What stood out most were the physiological effects of restraint, which triggered stress and elevated heart rates that masked or distorted drug responses. For example, QTc intervals in restrained animals were shortened, which was directionally wrong compared to telemetry and hERG assay findings with AMG 319 (see image). In dogs treated with AMG 337, the drop in blood pressure (telemetry) went undetected, likely because the animals had elevated sympathetic tone from handling related excitement. These discrepancies raise serious concerns about the value of restraint-based methods in toxicology studies, and their potential for misleading nonclinical CV risk assessment. The use of telemetry methods in toxicology paradigms would be a better and more reliable approach, especially if toxicology studies are the primary nonclinical in vivo data source for evaluating CV safety.
Image caption: AMG 319 exposure levels associated with QTc prolongation in non-human primates align with hERG channel inhibition and clinical observations. The telemetry-based data reinforced the clinical relevance of the NHP QTc data, whereas restraint-based methods erroneously detected QTc shortening. Red box: The clinical exposure range associated with QTc effects sizes of 30-60 ms.

The comment feature is locked by administrator.